


1Health, Medical and Neuropsychology Unit, Institute of Psychology, Leiden University, 2Leiden Institute for Brain and Cognition, Leiden, and 3Department of Psychiatry, Leiden University Medical Center, Leiden, The Netherlands
#Joint first authorship.
Itch and pain are important attention-demanding sensations that allow adaptive responses to potential bodily harm. An attentional bias towards itch and pain stimuli, i.e. preferential attention allocation towards itch- and pain-related information, has been found in healthy, as well as in patient groups. However, it remains unclear whether attentional bias for itch and pain differs from a general bias towards negative information. Therefore, this study investigated attentional bias towards itch and pain in 70 itch- and pain-free individuals. In an attention task, itch- and pain-related stimuli, as well as negative stimuli, were presented alongside neutral stimuli. The results did not indicate an attentional bias towards itch-, pain-, and negative visual information. This finding suggests that people without itch and pain symptoms do not prioritize itch- and pain-related information above neutral information. Future research should investigate whether attention towards itch- and pain-related information might be biased in patients with chronic itch and pain.
Key words: attentional bias; pruritus; pain; cognitive processing.
Accepted May 26 2020; Epub ahead of print Jun 3, 2020
Acta Derm Venereol 2020; 100: adv00199.
Corr: Antoinette I. M. van Laarhoven, Leiden University, Faculty of Social and Behavioral Sciences, Institute of Psychology, Health, Medical and Neuropsychology Unit, PO Box 9555, NL-2300 RB Leiden, The Netherlands. E-mail: a.vanlaarhoven@fsw.leidenuniv.nl
Prevention of potential harm to the body is adaptive. Thus, people may preferentially allocate attention towards itch- or pain-cues, i.e. attentional bias. So far, research about this topic in itch is scarce and the evidence is mixed for pain. Therefore, more insight into the mechanism of attentional bias towards itch and pain is needed to demonstrate possible alterations in patients in a next step. The aim of this study was to investigate whether healthy individuals have an attentional bias towards itch and pain, which could not be demonstrated. Such attentional bias is perhaps particularly present in patients with chronic itch or pain.
In order to protect ourselves from potential harm, we allocate our attention preferentially to negative stimuli (e.g. an angry face or a picture of a snake). Thus, attentional bias (AB) towards these stimuli can occur (1). Acute itch and pain have a nocifensive function (2), i.e. they signal possible negative consequences (e.g. disease or injuries) and enable us to adapt our behaviour to prevent bodily harm. The assumption that itch demands attention is supported by studies of contagious itch, which show that people scratch themselves after seeing or hearing someone else scratching (3). Moreover, recent studies have shown that healthy people display an AB towards itch (4, 5). In pain research, studies have also supported that people show a small AB for pain, especially people who have chronic pain, although not all studies support this conclusion (6–8). The similarities in psychophysiology between itch and pain may imply similar exaggeration of AB in chronic itch (9, 10).
Concerning the underlying mechanism of AB towards itch and pain, it is unclear whether itch and pain demand attention only because of their negative valence or because there is a distinct AB specifically towards itch- and pain-related information on top of a general bias towards negativity. Moreover, it is unknown which aspect of attentional processing might be biased in relation to itch and pain. A possible candidate might be inhibition of irrelevant information (11, 12), because acute itch and pain can interrupt ongoing goal-directed behaviour that is unrelated to itch and pain. Therefore, higher general ability of attentional inhibition might be related to less AB towards itch and pain, which is indeed suggested by some earlier studies (13, 14). In addition, there are other characteristics that may explain individual differences in AB towards itch and pain, such as neuroticism and catastrophization, which have shown associations with itch and pain, respectively, in some studies (3, 7, 14, 15).
Experimental methods to assess AB towards itch and pain have made use of different stimulus material, but, to our knowledge, there is no consensus as yet about which material works best (4, 7). From an evolutionary perspective, visual itch and pain cues can enable protective behaviour by signalling threat. Therefore, visual material, like words or pictures, are a representative choice that have been most frequently applied and appear to be most ecologically valid, except for the somatosensory perception itself (4, 7).
To the best of our knowledge, AB towards itch, pain and negative information has not yet been investigated within a single healthy sample, despite many similarities in psychophysiology and protective function (9). Therefore, the current study investigated AB towards itch- and pain-related printed words and pictures in itch- and pain-free individuals. Specifically, it was hypothesized that itch- and pain-related stimuli draw more attention, as opposed to concurrently presented neutral stimuli. It was also hypothesized that there is a stronger AB towards itch and pain than towards solely negative stimuli. Furthermore, this study explored whether more attention towards itch- and pain-related stimuli is related to general attentional inhibition and self-reported individual characteristics, e.g. pain catastrophizing and attention towards bodily sensations.
Participants
The sample comprised 70 itch- and pain-free volunteers. Power calculations using a power of 0.90 and an alpha of 0.05 yielded a targeted sample size of 63 plus 10% possible data loss, based on a previous study using a similar behavioural attention task (i.e. dot-probe task) for itch that found a Cohen’s d of 0.45 (4).
Participants had to be between 18 and 30 years old and fluent in the Dutch language. Exclusion criteria for participants were: current itch or pain levels >3 on a scale from 0 (“no itch/pain”) to 10 (“worst imaginable itch/pain”), diagnosis of any chronic pain condition (e.g. rheumatoid arthritis), chronic itch condition (e.g. eczema) or psychiatric disorder (e.g. major depression, AD(H)D). Participants were recruited through the Leiden University Research Participation system (SONA Systems Ltd, Tallinn, Estonia) and social media (e.g. Facebook), and all participants provided written informed consent. The local ethics review committee of the institute of Psychology of Leiden University approved the study (CEP16-1223/390).
Procedure
Written information about the study was sent to potential participants in which participants were informed that the aim of the study was to investigate people’s responses to visual itch- and pain stimuli. Potential participants were screened via the online system Qualtrics (Provo, UT, USA). Screening consisted of questions about demographics, psychiatric diagnoses and chronic itch and pain, as well as visual analogue scales on itch, pain and fatigue. A battery of self-report questionnaires was also included. Eligible participants were invited to the laboratory at the Faculty of Social and Behavioral Sciences at Leiden University for a testing session of approximately 50 min. Participants were instructed not to take medication and drugs, or more than 4 glasses of alcohol <24 h before the test session, and not to consume any food or drinks containing caffeine <1 h before the test session. After a brief explanation of the procedures and a check of inclusion and exclusion criteria, informed consent forms were signed. Participants indicated current levels of itch, pain and fatigue and thereafter a questionnaire on psychological distress was completed. During all tasks, participants were positioned in front of the computer monitor with their heads in a chin rest throughout testing (distance approximately 50 cm). Participants then started with an attentional inhibition task, followed by 2 tasks that assessed AB towards itch, pain and negative stimuli. The order of the 2 AB tasks was randomized, stratified by gender (www.randomization.com). Instructions were presented on the screen before the start of each task and summarized orally by the researcher. After performance of all tasks, participants rated the applicability to itch and pain of a selection of the stimuli. Lastly, participants were debriefed and received monetary reimbursement or research participation credits (as part of Leiden University’s undergraduate programme).
Attention tasks
All tasks were designed and administered using E-Prime 2.0 with Microsoft Windows 7 and a Philips Brilliance 220B TFT screen (Resolution 1,280 × 1,024, 60 Hz). Custom-made finger buttons (Pushbutton Switch, SPDT, Off-(On)) were connected to a Serial Response Box at a fixed position on the table to collect participants’ response (Psychology Software Tools, Inc., Sharpsburg, PA, USA).
Dot-probe tasks. Two dot-probe tasks were administered to measure AB for itch- and pain-related words and pictures (7, 16). In these tasks, participants were instructed to respond to the orientation of 2 small dots appearing after the presentation of a word pair (i.e. dot-probe task with words) or after the presentation of a picture pair (i.e. dot-probe task with pictures). AB is defined as faster reaction times on trials when the dots appear at the location of the nocifensive (itch, pain or negative) stimuli (i.e. congruent trial) than at the location of the neutral stimuli (i.e. incongruent trial).
For the dot-probe task with pictures, 20 itch- and 20 pain-picture pairs consisted of, respectively, one itch- and pain-related image paired with one neutral image, half of these depicting either skin or objects (e.g. a coffee mug). Itch-related images showed hands scratching the skin of various body parts (e.g. neck, back, legs). Pain-related images depicted hands putting pressure on the skin of various body parts or supporting joints. Neutral skin images featured the same body parts without any hands. In all these images, it was made sure that the skin was free of marks that could be related to pain or itch (e.g. red spots, bruises, cuts). The hands in the images were positioned on top of bare skin or on clothes without bright colours or patterns. Ten negative picture pairs consisted of a negative image (e.g. garbage, skull) and a neutral object image. Pictures were matched in colour and brightness as much as possible. All pictures were 256×256 pixels and were displayed on a black background.
For the dot-probe task with words, 20 itch-, and 19 pain- (one pair was used twice by accident), and 10 negative (i.e. affective) words were paired with neutral words. The affective words were somatosensory pain words (e.g. throbbing), associative pain words (e.g. infection), somatosensory itch words (e.g. itching), associative itch words (e.g. eczema), and negative words (e.g. bomb). Neutral words (e.g. clock, pillow) were matched in length and syllabi to the nocifensive words, as well as on word type (adjectives or nouns). Stimulus words were presented in bold white lowercase letters (Courier New font, size 26 pt) on a black background.
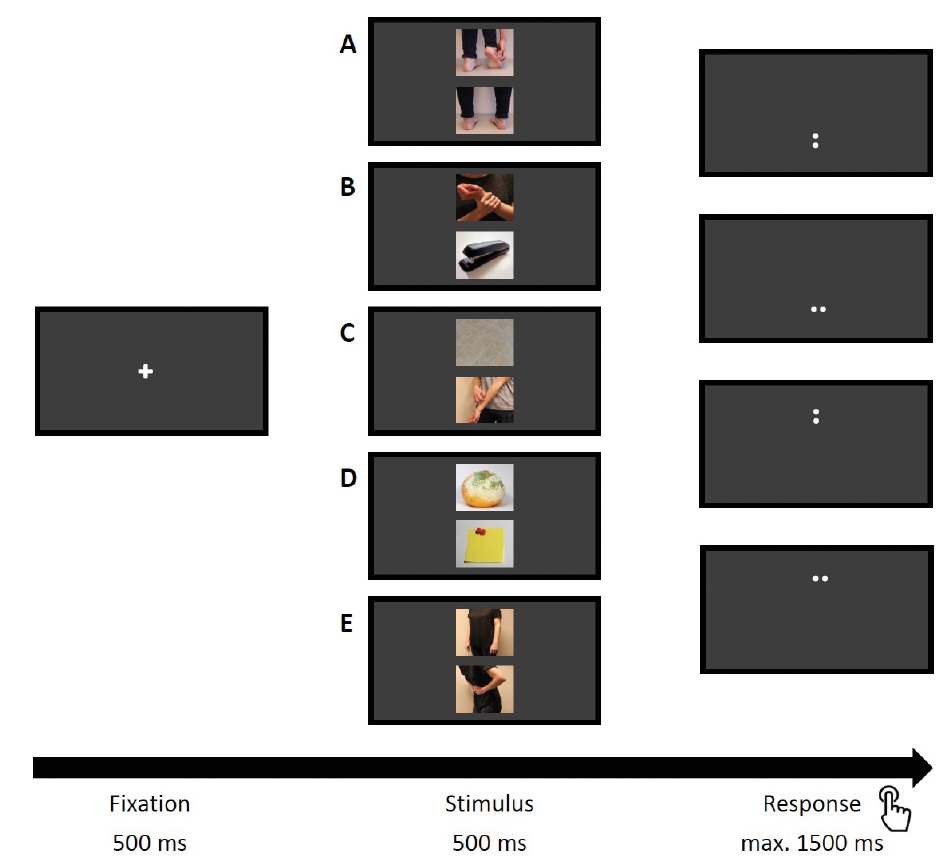
Each trial started with the appearance of a central fixation cross for 500 ms, followed by a stimulus pair presented above each other at the 20% and 80% (height) position on the screen with the fixation cross in between, at 50%, all centred in the middle of the screen (50% width). Stimulus pairs were displayed for 500 ms, where after 2 dots appeared at the upper or lower stimulus location for a duration of 1,500 ms maximum as response targets. These dots were either horizontally or vertically oriented and were equally likely to appear at the location of the neutral stimulus or the nocifensive stimulus. Hand side and dots orientation mapping was counterbalanced across participants. The stimulus pairs were presented in random order and each pair appeared 4 times, twice with the nocifensive stimulus on the top (bottom) of the screen and twice with the dots oriented horizontally (vertically). Fig. 1 displays one trial of the dot-probe task with pictures and shows examples of each picture pair. In order to reduce potential habituation effects to the itch-, pain- and negative stimuli, additional filler trials were included showing pairs of only neutral pictures (20 trials of neutral object pairs and 20 trials of neutral skin pairs) or neutral words (20 trials in total) (17). Both dot-probe tasks started with a practice phase of 16 trials including feedback on performance, followed by 2 first trials containing 2 neutral stimuli. The test phase consisted of 240 trials in the dot-probe task with pictures and 220 in the dot-probe task with words. Blocks of 40 trials were separated by breaks of 30 s. Each task took approximately 6 min to complete. Accuracy and reaction times (RTs) to respond to the orientation of the dots were recorded for each trial.
Fig. 1. One trial of the dot-probe task with pictures. Examples of each picture pair (A=itch – neutral skin; B=pain – neutral object; C=itch – neutral object; D=negative – neutral object; E=pain – neutral skin) and each of the 4 response windows are shown. Note: proportions of pictures to the screen were adjusted to enhance the visibility of the pictures.
Validation of the dot-probe stimulus material. Based on a consensus on face-validity by 4 researchers, 50 pain-related images, 54 itch-related images, 118 neutral images of skin, 120 neutral images of objects, 36 negative images, 75 pain-related words, 66 itch-related words, 215 neutral words, and 55 negative words were preselected for validation.
These preselected words and pictures were subsequently rated in random order in an online questionnaire via Qualtrics by a sample of 28 individuals (9 males, 19 females, age range 25-67 years). The sample consisted of 6 healthcare professionals, 19 patients with chronic itch/pain and 3 people from the general population without chronic itch or pain. Participants were reimbursed by taking part in a lottery for a gift voucher (4× €25).
Based on these ratings, the whole validated set includes 40 itch-related images and 46 itch-related words, as well as 38 pain-related images and 45 pain-related words. In addition, 108 neutral images of objects, 108 neutral images of human skin, and 110 neutral words were selected for the overall validated set. Lastly, 10 negative images and 11 negative words were included. A subset of this validated set was used in the current study. Ratings for the selected stimuli in the different stimulus categories, as well as more details on the validation ratings can be found in Appendix S1 and Table SI).
Flanker task. The Flanker task was used to measure attentional inhibition of task-irrelevant information (18). Each trial started with the appearance of a fixation cross for a duration of 500 ms, after which a set of 5 numbers was shown. The number in the centre was flanked either by the same stimuli in congruent trials (“44444” or “22222”) or by different stimuli in incongruent trials (“44244” or “22422”). The complete task consisted of 8 practice trials and 2 blocks of 60 experimental trials with a self-determined break in between. Congruent and incongruent trials were presented randomly, but equally distributed across the 2 blocks. Participants were instructed to indicate as quickly as possible whether the number in the centre was the number 2 or the number 4. The task lasted approximately 5 min, and accuracy and RTs to respond to the stimulus in the centre were measured.
Questionnaires
All questionnaires were presented via the online system Qualtrics (Provo, UT, USA).
Psychological distress was measured to confirm that all participants were healthy as was intended. This was measured with the Depression, Anxiety, and Stress Scale – short form (DASS-21; 19). Cronbach α for the subscales depression, anxiety, and stress were, respectively, 0.78, 0.63, and 0.79. To assess individual characteristics that are possibly related to AB the following questionnaires were used: attentional disengagement from bodily sensation, i.e. itch, pain, and fatigue was assessed with 3 Likert scales, ranging from 1 (not at all) to 5 (always). Attentional focus on bodily sensations was measured with the Body Vigilance Scale (BVS; 20), Cronbach α 0.71. Attentional focus on pain and itch was assessed with, respectively, the Pain Vigilance and Awareness Scale (PVAQ; 21), Cronbach α 0.91, and the PVAQ adjusted for itch (PVAQ-I; 4), Cronbach α 0.89. Catastrophizing was assessed with the Pain Catastrophizing Scale (PCS; 22), Cronbach α 0.92, and PCS-adjusted for itch (PCS-I; 4), Cronbach α 0.88. Cognitive intrusion was measured with the Experience of Cognitive Intrusion of Pain (ECIP; 23; and the ECIP-adjusted for itch (ECIP-I; 4), both Cronbach α 0.96. Neuroticism was measured with the subscale Neuroticism of the Eysenck Personality Questionnaire – revised short form (24), Cronbach α 0.77.
Lastly, a subset of stimuli (20 neutral skin-, 20 itch-, 20 pain- pictures and 20 itch- and 20 pain-words) was rated on a Likert scale ranging from –4 (applicable to intense pain) to 4 (applicable to intense itch) with 0 labelled as neutral. Table SII displays the minimum and maximum obtainable scores for each questionnaire.
Statistical analyses
Data for the attention tasks were extracted with E-DataAid (Psychology Software Tools, Inc., Sharpsburg, MD, USA). For the dot-probe tasks, RTs >150 were extracted and for the Flanker task RTs between 150 and 1,500 ms. As accuracy rates of all participants were high and above 70%, all cases were included in the analyses (4, 16). Statistical analyses were performed using SPSS 23 (IBM SPSS Statistics, Armonk, NY, USA). Data on RTs were normally distributed. One participant showed outlying RTs for the Flanker task, as well as for negative trials of the dot-probe task with words (step of 1.5 × interquartile range). Therefore, analyses were performed both including and excluding data of this participant. For the dot-probe task for words and the dot-probe task for pictures separately, differences in RTs on congruent and incongruent trials per stimulus type were investigated by means of a 3 (stimulus type: itch, pain, negative) × 2 (congruency: congruent vs incongruent) repeated measures analysis of variance (RM-ANOVA) with both factors as within-subjects factors. Of interest was the main effect of congruency, as well as the stimulus type by congruency interaction. For stimulus type, planned contrasts were defined to specifically assess responses on itch and pain vs negative trials, as well as responses on itch vs pain trials. For the Flanker task, RTs between congruent and incongruent trials were compared in a RM ANOVA with congruency (congruent vs incongruent) as within-subjects factor.
Additional exploratory analyses were performed on the dot-probe task data by exploring whether RTs on the itch-neutral and pain-neutral stimulus pairs in the dot-probe task with pictures differed when the neutral image depicted skin or objects. A 2 (neutral picture type: skin vs object) × 2 (congruency: congruent vs incongruent) RM ANOVA was performed separately for itch- and pain- trials. Secondly, for the dot-probe task with words, differences in RTs between trials with associative and somatosensory words were explored by means of a 2 (word type: associative vs sensory) × 2 (congruency: congruent vs incongruent) RM ANOVA for the itch and pain trials separately.
AB indices were calculated using the following formula: RTincongruent – RTcongruent for each stimulus type for both dot-probe tasks (4, 8). In the same way, a Flanker congruency index was calculated. A higher and positive AB index represents more AB towards itch, pain or negative stimuli and a higher Flanker congruency index represents stronger attentional inhibition. Correlations between AB indices and the Flanker congruency index, as well as outcomes of self-report questionnaires were explored, to investigate whether AB towards itch or pain is associated with attentional inhibition and individual characteristics (e.g. neuroticism, catastrophizing). An alpha of 0.05 was considered statistically significant for all statistical tests and for the results of the RM ANOVA generalized eta-squared was calculated as a measure of effect size (25).
The final sample of 70 participants consisted of 47 females and 23 males and had a mean age ± standard deviation (SD) of 21.9 ± 2.1 years, see Table SII for descriptive statistics of individual characteristics. As intended, the DASS-21 confirmed that participants were not substantially depressed, anxious or stressed before testing. Table SIII presents the itch and pain intensity ratings for the stimulus material of both dot-probe tasks.
Dot-probe tasks
Similar mean accuracy scores were obtained for the congruent and incongruent trials in both dot-probe tasks; 93% (range 83–98%) for the dot-probe task with pictures and 92% (range 78–99%) for the dot-probe task with words. Mean RTs per trial type of both dot-probe tasks are presented in Fig. 2 and in Table I.
Fig. 2. Mean reaction times, in ms, per trial type of the dot-probe tasks with (A) pictures and (B) words. Error bars represent standard error of the mean (n =70).
Table I. Reaction times (RT), in ms, per trial type of the dot-probe tasks with pictures and words (n = 70)
Dot-probe task with pictures. The main hypothesis of an AB towards itch and pain could not be confirmed, as the stimulus type by congruency interaction was not significant, F(2,138)=0.306, p = 0.737, ηG2=0.002. Planned contrast showed no significant differences in RTs on congruent and incongruent trials between itch and pain trials in comparison with negative trials (p > 0.05). In addition, there were no differences in RTs on congruent and incongruent trials between itch and pain trials (p > 0.05). A tendency towards significance was observed for the main effect of congruency, F(1,69)=3.77, p = 0.056, ηG2=0.011, with incongruent trials being faster than congruent trials. Furthermore, results showed a significant main effect of stimulus type, F(2,138)=12.94, p < 0.001, ηG2=0.068. Planned contrasts indicated that participants responded overall significantly faster on itch and pain trials compared with negative trials (p < 0.001), but there was no significant difference in RTs between itch and pain trials (p > 0.05). Exclusion of the outlier did not change the significance levels of the results.
Dot-probe task with words. There was no AB found towards itch and pain words; the interaction of stimulus type and congruency was not significant, F(2,138)=1.87, p = 0.158, ηG2=0.011. Planned contrast showed no significant results (p > 0.05). No significant difference was found between the congruent and incongruent trials, F(1,69)=0.13, p = 0.718, ηG2=0.0003. However, a significant main effect of stimulus type was found, F(2,138)=3.08, p = 0.049, ηG2=0.019. Planned contrasts showed faster overall RTs on pain trials compared with itch trials (p < 0.05), but no significant differences in responses on itch and pain trials compared with negative trials (p > 0.05). After exclusion of the outlier, the main effect of stimulus type was no longer significant, but a tendency towards significance remained F(2,68)=2.91, p = 0.058, ηG2=0.019.
Attentional bias indices. For the dot probe task with pictures, mean ± SD AB indices for itch, pain and negative pictures were –4.2 ± 24.2, –2.1 ± 27.6, and –6.3 ± 40.6, respectively. For the dot probe task with words, mean ± SD AB indices for itch, pain and negative words were –1.3 ± 24.0, –3.0 ± 27.3, and 6.4 ± 36.1, respectively.
Exploration of effect of neutral picture types. For itch trials, no significant differences were found in RTs between trials with itch-skin and itch-object picture pairs, F(1,69)=2.21, p = 0.142, ηG2=0.008. Similarly, in pain trials no significant differences were found in RTs between trials with pain-skin and pain-object picture pairs, F(1,69)=0.46, p = 0.502, ηG2=0.002. Moreover, the interaction between neutral picture type (skin vs object) and congruency (congruent vs incongruent) was not significant for itch trials, F(1,69)=0.91, p = 0.341, ηG2=0.005, or for pain trials, F(1,69)=0.01, p = 0.943, ηG2=0.00003. Means and standard deviations for RTs on trials with skin vs object pictures can be found in Table SIV.
Exploration of effect of word types. Results neither indicated significant differences in RTs between trials with associative and sensory itch words, F(1,69)=0.22, p = 0.640, ηG2=0.0009, nor between trials with associative and sensory pain words, F(1,69)=0.82, p = 0.370, ηG2=0.006 Also, no significant interaction between congruency and word type was found in itch trials, F(1,69)=1.21, p = 0.274, ηG2=0.006, and in pain trials, F(1,69)=0.54, p = 0.466, ηG2=0.007. Table SIV presents means and SD for RTs on trials with associative and sensory itch and pain words.
Flanker task
On average, participants responded correctly on 95.5% (range 82–100%) of all trials of the Flanker task. Results showed a significant main effect of congruency, F(1,69)=265.845, p < 0.001, ηG2=0.111, indicating faster RTs on congruent (411.76 ± 59.79 ms) compared with incongruent trials (452.34 ± 55.56 ms). Exclusion of the outlier did not change the significance of the results. The mean ± SD congruency index was 40.59 ± 20.83 (31.35–80.40).
Correlation between attentional bias indices with individual characteristics
No significant correlations were observed between AB indices for itch and pain in the dot-probe tasks and outcomes of self-report questionnaires on individual characteristics. With regards to the correlation between AB indices and attentional inhibition, there were also no significant correlations. See Table SV for the correlation matrix.
The current study did not provide evidence for the presence of an AB towards itch, pain and negative pictures and words in healthy participants. However, responses on trials with itch- and pain pictures were overall faster than on trials with negative pictures, suggesting that particularly general negative information, unrelated to itch or pain, slowed down attentional processing in the current sample. The results of the current study are in contrast with earlier findings, demonstrating an AB towards visual itch cues in healthy individuals (4, 5), and add to the evidence that there is no AB towards pain cues in healthy individuals, as already suggested by meta-analyses (7, 8).
Van Ryckeghem & Crombez (6) suggest approaching AB from a motivational account of attention towards pain, which states that attention is only biased towards pain if pain is related to someone’s current goals (26). Within their proposed framework, it seems reasonable that itch- and pain-free individuals show no AB towards stimuli that are unrelated to the task goal, i.e. it was not essential to focus on the visual stimuli in the current design for good task performance. However, this does not explain previous findings of AB to itch in healthy individuals in research using a similar design (4). Moreover, from a dysfunctional information processing account, it is suggested that visual material does not sufficiently activate pain schemas in healthy individuals, because seeing someone in pain does not usually induce pain in the viewer (although research has shown that pain can be vicarious, i.e. people empathize with someone in pain (27)), which could be an additional reason that people whose current goal is unrelated to pain, i.e. healthy individuals show no AB towards pain (6). However, this explanation does not apply to itch, because itch can elicit itch in the observer, i.e. itch is contagious (3, 28).
The absence of an AB towards itch-related, pain-related, and negative pictures in the current study might be related to the neutral skin and neutral object pictures. First of all, the neutral skin pictures depicted the same person in the same posture as in the itch- and pain pictures, but without a scratching or painful gesture (see Fig. 1 for examples of these picture pairs). It is possible that more effort is required to process and interpret a picture of a gesture, but this is not in line with findings showing that attention is more easily drawn to action-related vs static (i.e. a gesture vs no gesture) pictures (29). Furthermore, it might also be that object pictures draw more attention because they are easier to process and interpret than the more complex itch- and pain pictures. Altogether, these concerns cannot exclusively explain the current findings, because earlier studies on itch used comparable itch-related and neutral pictures and did show an AB towards itch in healthy volunteers (4, 5). Moreover, the itch and pain stimuli (words and pictures) were rated rather low on itchiness and painfulness in the current study. Notably, using intense itch and intense pain as anchor points probably explains lower ratings than during the validation process (with anchors ”How applicable is this stimulus to itch and pain”).
The results of the current study demonstrate no AB towards itch-related and pain-related words, or towards negative words. Words were often used in earlier research in AB towards itch and pain, and these words were rather similar to our stimuli. Moreover, the neutral words were not different in aspects other than the relatedness to itch or pain (e.g. matched on length, word type). Because we know that itch is contagious when people talk about itch (3), we would assume that these kind of words would draw attention towards their location. However, for pain, a previous meta-analysis has shown that only sensory pain words elicit an AB towards pain in healthy people, compared with affective and associative pain words, although there were only a few studies that included associative words (7). This is in contrast to the current results, which could not support such a difference in AB towards sensory or associative words, either for itch, or for pain. Nevertheless, the existing evidence at this point is too limited to draw definitive conclusions about potential differences in AB towards sensory or associative itch- and pain-words.
In general, no associations were found between the measured individual characteristics, including attentional inhibition, and AB for itch, pain and negativity. This finding is mostly in line with earlier studies on itch and pain (4, 7, 16), except for previous studies reporting significant associations between AB for pain and attentional inhibition and/or attentional control (33–35). However, as healthy individuals in the current study did not show an AB towards itch and pain in the first place, it is difficult to draw firm conclusions about their possible association with other characteristics.
Studies on AB towards itch and pain were, so far, not able to specify at which time point in attentional processing an AB might occur. Still, in recent meta-analyses, results suggest that different display times (e.g. 500–1,000 ms vs >1,000 s) elicit an AB towards pain stimuli or not (7, 8). This suggests that display time of stimulus material is a key parameter to investigate in AB research. More research is needed to investigate early orienting of attention (e.g. presentations of 20 ms) or later disengagement of attention (e.g. presentations of >1,000 ms).
In line with a motivational account (6), as described above, it is important to note that people who have itch or pain for a prolonged time probably react differently to itch- and pain-related stimuli in their environment. This has, indeed, been shown in pain research (6, 7), as well as in itch research (5). In patients, dealing with their itch- and pain-symptoms might become a goal on its own, which can lead patients to focus even more on itch and pain. It appears reasonable therefore to assume that itch- and pain-related information is more relevant and more salient for patients who are daily confronted with and disrupted by these symptoms. Future research could, for instance, include priming for itch and pain to increase saliency and relevance in a healthy sample, although research in patients is also still desirable.
For further research, we propose that different stimulus material should be continued to be investigated. Also, other presentation times should be included (e.g. 20 or >1,000 ms) and besides behavioural measurements, physiological measurements, such as eye-tracking and electro-encephalography may be more sensitive for investigating the time course of attention allocation towards itch and pain, assuming that attention fluctuates during the presentation of a stimulus (30, 31). Although this study could not find any self-reported predictors of AB, future studies could examine other components of attention, such as attentional control (13) to potentially shed more light on the mixed results of the different studies on AB performed so far. Lastly, a more heterogeneous sample concerning gender, age and education level is desirable to enhance generalizability to the broader population.
In conclusion, the current study does not support the presence of AB towards representations of itch and pain in itch- and pain-free individuals. Nonetheless, this study leads to future directions to further elucidate the different components of attention allocation towards itch- and pain-related visual cues in healthy individuals and, most importantly, recommends future research on AB in patient groups.
The authors would like to thank Elisa Kovacs for her support with the selection and validation of the stimulus material; Fabiënne van den Ende and Hanna Jagt for their contribution to the data collection, and Maureen Meekel and Stephen Brown for technical support and programming of the attention tasks. This research is supported by an Innovation Scheme (Veni) Grant (451-15-019) of the Netherlands Organization for Scientific Research (NWO), granted to A.I.M. van Laarhoven.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize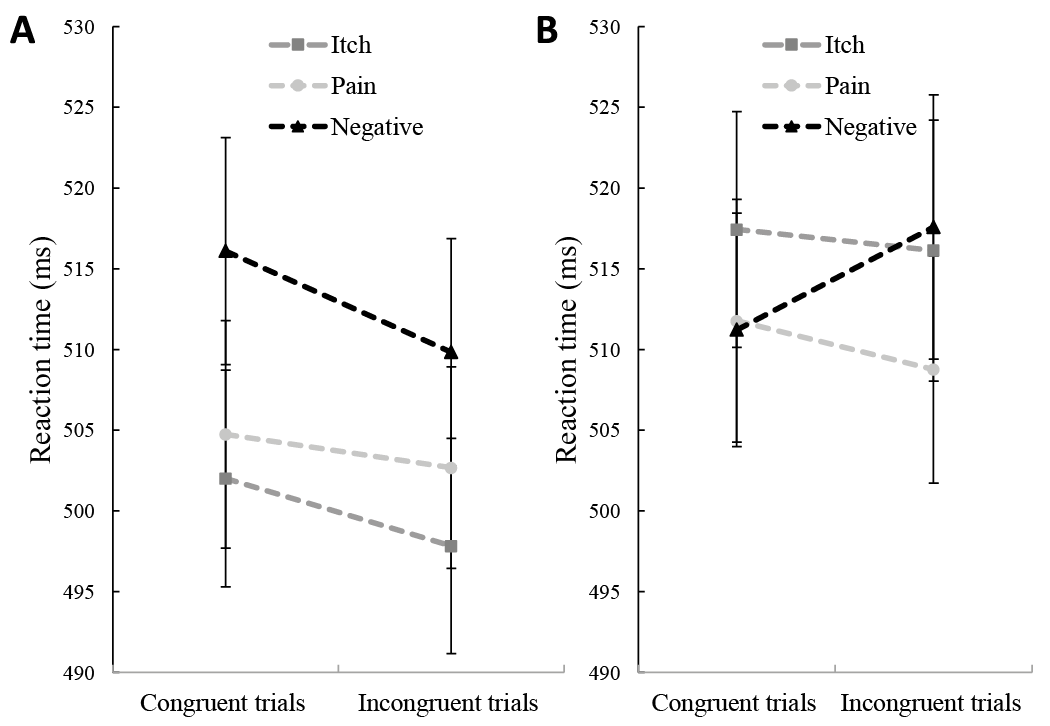 Click to show fullsize
Click to show fullsize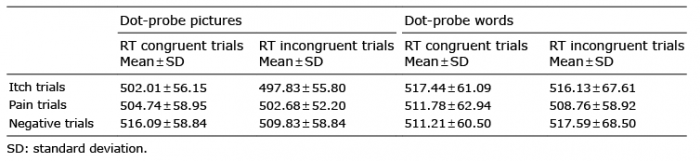 Click to show fullsize
Click to show fullsize